

.jpg)




— reducing the high number of false diagnosis of kidney stones
By Dr. Vijai Persaud
MMED Diagnostic Radiology
KIDNEY stones (also called renal calculi or nephrolithiasis) refer to the formation of hard pebble-like deposits made of salts and minerals inside the kidneys. The lifetime risk of nephrolithiasis is approximately 11 per cent for men and seven per cent for women. Accurate detection and measurement of renal calculi is important to guide in management decisions. Commonly used diagnostic tests include ultrasound, CT scan and x rays. There are advantages and disadvantages of each.
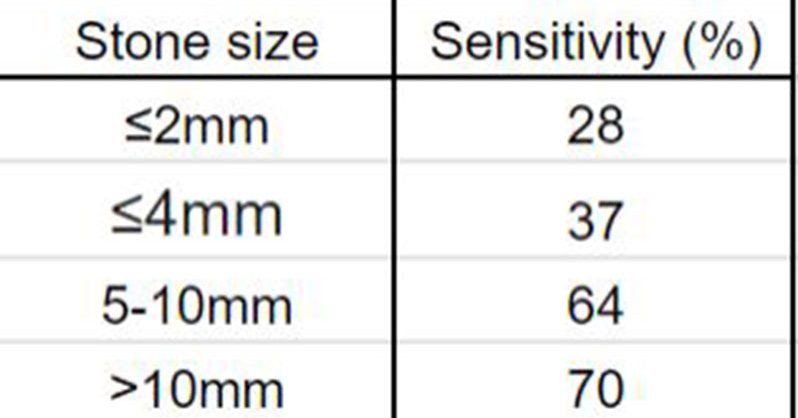
Ultrasound (USG) is an easily accessible, relatively inexpensive imaging method that uses high-frequency sound waves to characterise tissue. Ultrasound should be used as the initial diagnostic imaging test, with further imaging studies performed at the discretion of the physician on the basis of clinical judgment. It has the ability to demonstrate stones, hydronephrosis (swelling due to obstruction), renal inflammation, ruptured fornices, ureteric jets, mass and abscess. Stones that are located close to the corticomedullary junction, particularly when small, can be difficult to reliably identify. The sensitivity of USG in detecting kidney stones is low when compared with CT. While this improves with increasing stone size, it is widely known that ultrasound misses approximately a ¼ of large-sized stones (>10 mm) and nearly 3/4 of stones not visualised were transducer settings and focal distance.
 In many cases it is difficult to determine whether a urinary stone is present due to its indistinct echogenicity and indiscrete or poor posterior acoustic shadowing. The twinkle artifact sign that can be seen on colour flow doppler ultrasound is also helpful when present. In addition, given the variety of settings and techniques, USG is more operator-dependent than CT. Indistinct echogenicity of stones results from surrounding echogenic tissue which may include bowel, prominent renal sinus fat and mesenteric fat. The echogenic appearance of these tissues can frequently produce acoustic shadowing which can be erroneously interpreted as renal stones. Renal artery calcifications should also be taken into consideration, especially in patients with long-standing diabetes, hypertension, or other systemic diseases associated with atherosclerotic vascular disease. Why is this of concern? It leads to inaccurate diagnosis or overcalling of kidney stones. This causes unnecessary patient anxiety, triggers unwarranted follow up ultrasound examinations and potentially misleads the managing doctor. The ensuing financial burden is also evident. Many patients, being concerned about their diagnosis, would have frequent ultrasound examinations. Studies have shown that as a result, one in five patients may be inappropriately managed when using USG alone.
In many cases it is difficult to determine whether a urinary stone is present due to its indistinct echogenicity and indiscrete or poor posterior acoustic shadowing. The twinkle artifact sign that can be seen on colour flow doppler ultrasound is also helpful when present. In addition, given the variety of settings and techniques, USG is more operator-dependent than CT. Indistinct echogenicity of stones results from surrounding echogenic tissue which may include bowel, prominent renal sinus fat and mesenteric fat. The echogenic appearance of these tissues can frequently produce acoustic shadowing which can be erroneously interpreted as renal stones. Renal artery calcifications should also be taken into consideration, especially in patients with long-standing diabetes, hypertension, or other systemic diseases associated with atherosclerotic vascular disease. Why is this of concern? It leads to inaccurate diagnosis or overcalling of kidney stones. This causes unnecessary patient anxiety, triggers unwarranted follow up ultrasound examinations and potentially misleads the managing doctor. The ensuing financial burden is also evident. Many patients, being concerned about their diagnosis, would have frequent ultrasound examinations. Studies have shown that as a result, one in five patients may be inappropriately managed when using USG alone.
Sensitivity of Ultrasound by kidney stone size. (BJU)
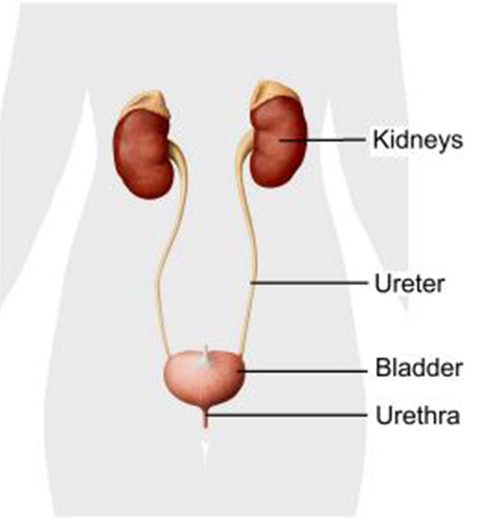 In contrast, gallstones and urinary bladder stones are easily identified using ultrasound due to the presence of surrounding fluid (bile and urine). CT scan has a higher accuracy in the diagnosis of small stones. It has the advantage whereby not only are the kidneys evaluated for stones, but the entire genitourinary system i.e the ureters and bladder also. It is used in the emergency setting for diagnosis and in the surgical setting due to its higher level of anatomical detail which is essential for surgical management. The main disadvantages are the cost and radiation exposure. The radiation dose however can be decreased by using low-dose protocols. This method uses specific protocols resulting in lower tube current. Stones depending on their sizes can sometimes get stuck within the ureters as they descend to the bladder. If they remain there for a long period, it can result in obstruction. The ureters can dilate and eventually it also happens to the kidneys. This in medical terms is called hydronephrosis or ureterohydronephrosis. If a stone remains in that location for a long period of time it may damage the kidney if it is not treated. Consultation with your doctor or urologist would be important to determine the appropriate management, so as to prevent long-term kidney damage. Abdominal X Rays also referred to as Kidney, ureter, bladder (KUB) is most helpful in evaluating interval stone growth in patients with known stone disease. It is less helpful in the setting of acute stones and is largely being replaced by ultrasound and CT. In summary, although ultrasound is an ideal imaging method for renal pathology and complications, it has low sensitivity for detecting small stones and increased awareness of this is important to avoid false diagnosis. In uncertain cases, a low dose CT scan can provide accurate information.
In contrast, gallstones and urinary bladder stones are easily identified using ultrasound due to the presence of surrounding fluid (bile and urine). CT scan has a higher accuracy in the diagnosis of small stones. It has the advantage whereby not only are the kidneys evaluated for stones, but the entire genitourinary system i.e the ureters and bladder also. It is used in the emergency setting for diagnosis and in the surgical setting due to its higher level of anatomical detail which is essential for surgical management. The main disadvantages are the cost and radiation exposure. The radiation dose however can be decreased by using low-dose protocols. This method uses specific protocols resulting in lower tube current. Stones depending on their sizes can sometimes get stuck within the ureters as they descend to the bladder. If they remain there for a long period, it can result in obstruction. The ureters can dilate and eventually it also happens to the kidneys. This in medical terms is called hydronephrosis or ureterohydronephrosis. If a stone remains in that location for a long period of time it may damage the kidney if it is not treated. Consultation with your doctor or urologist would be important to determine the appropriate management, so as to prevent long-term kidney damage. Abdominal X Rays also referred to as Kidney, ureter, bladder (KUB) is most helpful in evaluating interval stone growth in patients with known stone disease. It is less helpful in the setting of acute stones and is largely being replaced by ultrasound and CT. In summary, although ultrasound is an ideal imaging method for renal pathology and complications, it has low sensitivity for detecting small stones and increased awareness of this is important to avoid false diagnosis. In uncertain cases, a low dose CT scan can provide accurate information.




