

.jpg)





“IMAGINE falling and hitting a sensitive spot on your body, pulling out a tooth without anaesthesia and stumping your little toe on the corner of a table. It’s worse than that put together,” Suzanne-Abigail Claxton said as she painted a vivid picture of the excruciating pain she experiences as a sickler. “When those things happen, the pain is just for a short while. With a crisis, it goes from zero to 100 real quick and stays there. The pain doesn’t ease; the pulsating pain just stays. There is no comfortable position; every move you make is torture. Sometimes you can manage with the pain. Other times, you just want the pain to end NOW before you lose your sanity,” she said as she tried to contain tears welled up in her eyes.

At the tender age of two, Claxton who hails from the mining town of Linden, Region 10, was diagnosed with the full-blown Sickle Cell disease. It was only until she started crying out for pain in her joints that her parents realised that something was terribly wrong, but local doctors at the time could not ascertain her illness. It was a Cuban doctor who had recommended that she be tested for the Sickle Cell disease, and the result was shocking – it was positive.
According to the Guyana Sickle Cell and Thalassemia Association, the sickle cell disease is an inherited blood disorder, characterised mainly by chronic anaemia and periodic episodes of pain called “painful crises.” In the case of Claxton, she would have inherited an unusual gene (s) from both of her parents, and the two defective genes (SS) resulted in her developing Sickle Cell Anaemia. Prior to her diagnosis, her parents had no idea that they had the Sickle Cell trait.
“I am the eldest of four. The sister after me has Sickle Cell trait, the next sister has full-blown Sickle Cell like me and my brother has nothing. Both of my parents have Sickle Cell traits but they didn’t know until they found out that I have Sickle Cell,” she explained.
Today, Claxton is 26 years old. According to her, reaching adulthood was not an easy journey as it was filled with many stumbling blocks and countless days hospitalised at the Linden Hospital Complex.
“As a child and teenager, I had a lot of restrictions. I couldn’t do all the things that I wanted to, so that I could prevent going into a crisis. I couldn’t go swimming in the creek like others, I couldn’t get involved in the water wars that came with Phagwah, and I couldn’t do things that were too physically demanding,” she recalled.
There were many nights when she longed to attend basketball matches with her friends, but could not do so because the coldness of the atmosphere could have plunged her into a crisis. “I felt left out sometimes but I understood that it was for my own good.”
With adulthood, comes greater understanding, Claxton said, noting that she is now better able to manage her illness. “I’ve had to develop stress management or coping techniques, I try to keep warm in places that have AC or keep drinking lots of water when it’s really hot. Remembering to take all of my medication every day is also a part of my daily routine.”
She added: “All of these little elements are part of my lifestyle now. So I try as much as possible to avoid getting sick. When I do get sick I use medication I would have at home, drink extra water or use a hot-water bag on the areas that are hurting to ease the pain. If that doesn’t work, I go to the hospital for treatment.”
But also in adulthood come greater challenges, especially in the area of employment. Despite being the holder of nine CSEC subjects, five subjects at CAPE and a Bachelor’s in English with a minor in Communication from the University of Guyana (UG), she was forced to change several jobs, not because she is a poor worker, but because of her illness.

“When you’re sick you can’t get work done, so you’re seen as a liability sometimes. Some employers are more understanding than others. But finding the balance between earning a living and being healthy can be extremely difficult at times. It’s a matter of working within your means,” she noted. But she warned that one’s health must be given priority at all times. “Always put your health first and do what’s best for your health. If you’re not healthy, you can’t earn.”
Support
Thousands of sicklers die before reaching adulthood, and for this, Claxton said she is grateful to be alive, noting that her family and friends continue to give tremendous support.
“They have gone above and beyond for me in my good times and bad. My parents sacrifice sleep to take me to the hospital at 3 am or look after me while I’m hospitalised… I keep an amazing support system around me and they have made living with sickle cell easy.”
Meanwhile, in giving her own assessment of the ability of the public health care system to treat sicklers, Claxton opined that many of the public hospitals lack medication and simple apparatus needed to treat sicklers – a situation she says can be very frustrating, especially when you are in great pain.
“All hospitals should be able to give proper treatment to sicklers at all times. I know of a hospital that would be out of pain medication for months at a time.” But this is just the tip of the iceberg; she said some medical staff fail miserably in showing their compassionate side.
“Sicklers ought to be given top priority at the Emergency Room because a crisis means that there is a blockage in the blood vessels. Blockages mean organs will be deprived of oxygen, which is dangerous. The longer sicklers have to wait for treatment, the more damage is being inflicted. If sicklers could get ahead in the long lines at hospitals for treatment that would be great,” she told the Guyana Chronicle.
But Claxton is not the only one who believes that the local health care system can do more to help sicklers. Dr John Dickinson, who has been the medical officer for the Sickle Cell Association for approximately 15 years, said unfortunately many sicklers die before reaching adulthood, pointing out that just recently a toddler had succumbed to the disease.
“I know that Guyana is a Third World country, and so we are limited but even within the limitations of what we can do, very little is being done, especially in the area of activism.” According to him, the disease has to be dealt with on two levels, in the areas of treatment and prevention.
Newborn testing
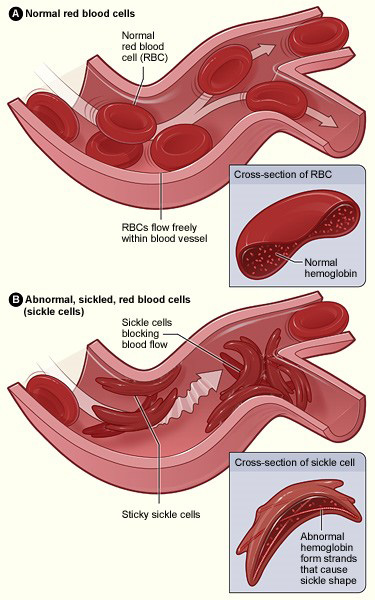
In the area of prevention, Dr Dickenson is of the strong belief that the Public Health Ministry should move to introduce newborn testing in the public health care system. It was explained that newborn screening is the process of testing newborn babies for some serious but treatable conditions such as the Sickle Cell disorder. This screening, which can be done by doing the “heel prick” test, would reveal whether a baby has normal red blood cells or sickled cells due to defective haemoglobin which causes the red blood cells to become stiff, thereby assuming the sickle shape.
“Once that child is found to be a carrier, that child grows up knowing that I am a carrier, the parents are now sensitised to the fact that they have produced a child that is a carrier or has the full-blown disease, and they would have to determine whether they will make more children, but the point is both parties will be empowered,” Dr Dickenson explained.
In alluding to developed nations such as England, he pointed out that it is mandatory for sicklers to be given 6-8 units of blood every two months. This allows them to maintain high levels of haemoglobin. Additionally, they conduct blood transfusion and bone marrow transplants which all come with price tags. These prices are not within the reach of many ordinary Guyanese; hence, Dr Dickenson said it will be prudent to do newborn testing so that affected babies can benefit from early available treatment.
Lack of clinics
Another sore area of concern, he said, is the lack of Sickle Cell clinics in Guyana. In fact in the entire country, there is one Sickle Cell clinic, which is located at the Linden Hospital Complex.
“We have tried for years to get one established at the Georgetown Hospital, but nothing has been done there,” he complained. These clinics, he emphasized, will help sicklers from going into crises. The most common of the crises is the painful crisis. “We have a clinic in Linden and it works, we have fewer patients going into crisis, because of the preventative measures we take,” he noted.
But with the establishment of clinics, Dr Dickenson said there is a need for haematologists or health personnel with training in Sickle Cell management, contending that there is no haematologist in Guyana. “I am not a haematologist… I just had specific training in Sickle Cell management in England, a very short programme in 2008.”
Meanwhile, Vice-President of the Sickle Cell and Thalassemia Association Nurse Grace Bond said the association has been trying its utmost to assist persons with Sickle Cell in Guyana by conducting outreaches, but complained that the Public Health Ministry needs to do more in the area of awareness. At its Charlotte and Alexander Streets, Georgetown location, the association facilitates a support-group meeting every second Saturday in every month starting at 14:00 hrs, but Nurse Bond said more awareness needs to be done.
The United Nations General Assembly in 2009 adopted a resolution for the recognition of Sickle Cell Anaemia as a public health problem. Sickle Cell Anaemia has been identified as one of the world’s foremost genetic diseases which has severe physical, psychological and social consequences for sicklers and by extension their families. As such, June 19 has been designated by the UN as World Sickle Cell Awareness Day.

“Since 2009, our country has not been highlighting this disease, and so I am asking this government to recognise that Sickle Cell is one of the worst genetic conditions.” In addition to acknowledging World Sickle Cell Awareness Day, the association would like the Public Health Ministry to establish a National Sickle Cell and Thalassaemia Register, implement guidelines and protocols of care, newborn screening, introduce a daily penicillin prophylaxis along with folic acid and introduce pneumovax from age two years for people with the Sickle Cell disease.
In playing its part, Nurse Bond pointed out that in 2014, the association held a road march in observance of World Sickle Awareness Day. Additionally, with the assistance of Guyanese designer Sonia Noel through her organisation Sonia Noel Foundation for Creative Arts, a fashion show was held in aid of the organisation.
Though the Sickle Cell Association has only 30 members, Nurse Bond said based on statistics garnered from the Georgetown Public Hospital and the Linden Hospital Complex, there are close to 500 persons with the Sickle Cell disease, noting that persons from across the country journey to these facilities to seek treatment.
Gov’t pledges support
Health Minister Dr George Norton, in acknowledging that there might have been some oversight in giving due recognition to World Sickle Cell Awareness Day, pledged his ministry’s commitment to strengthen its relationship with organisations such as the Guyana Sickle Cell and Thalasasemia Association.
“Certainly they will get our support,” he said. In addressing the issue surrounding the Sickle Cell Disorder, Dr Norton said the Public Health Ministry has recently secured Argentina’s commitment to assist in the area of haematology.
“Haematology is Argentina’s area of strength, and so we have requested post-graduate programmes in the area of haematology, blood transfusion and the production of blood products,” he disclosed.
According to the World Health Organisation (WHO), approximately five per cent of the world’s population carry traits of haemoglobin disorders, mainly sickle-cell disease and thalassaemia.
An estimated 300,000 babies with severe haemoglobin disorders are born each year globally, and according to WHO, “the health burden of haemoglobin disorders can be effectively reduced through management and prevention programmes.”
In an effort to bring assistance to sicklers and persons living with haemoglobin disorders, the WHO has adopted two resolutions. The resolution on Sickle Cell disease was adopted during the 59th World Health Assembly in May, 2006, while the second resolution on Thalassaemia was adopted during the 118th meeting of the WHO Executive Board. These resolutions have called upon affected countries and the Secretariat of WHO to strengthen their response to these conditions. Additionally, a resolution on the prevention and management of birth defects, including Sickle Cell disease and Thalassaemia was adopted by the 63rd World Health Assembly in May 2010.




