–says filaria MDA supervisor
NINE pills. That’s the highest number of pills one would have to take as part of this year’s round of Mass Drug Administration (MDA) campaign to eliminate Lymphatic Filariasis as a public health issue.
For the past two years, the country has recorded significant coverage for this MDA, which seeks to remove Guyana as one of the four countries in the Caribbean which still has filaria as a public health issue. In fact, the coverage was recorded at 86 per cent in 2017, when the campaign was restarted, and 85 per cent last year when the campaign was in its second of five successive rounds. In order for the MDA to be successful, each round must record at least 65 per cent coverage.

“In previous years, we know that persons have become accustomed to the DEC [Diethylcarbamazine citrate] and the ALB [Albendazole] where you have the DEC killing the adult worms that causes filaria,” explained Dr. Annastacia Sampson, the National Supervisor for the MDA campaign for the Elimination of Lymphatic Filariasis.”
These tablets, however, work in conjunction over a period of five to six years to kill the parasitic worms, called nematodes, transmitted by the Culex mosquito in Guyana, which cause the disease. It is for this reason that the MDA requires five successive successful rounds.
RESOURCE-DEMANDING
According to Dr. Sampson, implementing five rounds can be “tedious”, since each round is resource-demanding and, expectedly, quite costly. Thus, the Ministry of Public Health, in addition to its partner, the Pan American Health Organisation- World Health Organisation (PAHO-WHO), has introduced a third drug to the regimen. This is Ivermectin, and it is distributed with the DEC and ALB as part of the new IDA drug regimen.
“With the use of Ivermectin, what will happen is that it will cut down the years that is needed for you to stop transmission, since the Ivermectin is known to kill and sterilise the adult worms that cause LF,” Dr. Sampson told the Guyana Chronicle.
Introducing the Ivermectin means that only two successive rounds of the IDA MDA are needed instead of the total five rounds required by the double-drug MDA. And as such, if the IDA MDA is successful this year, Guyanese will only have to take their ‘filaria pills’ once more, next year.
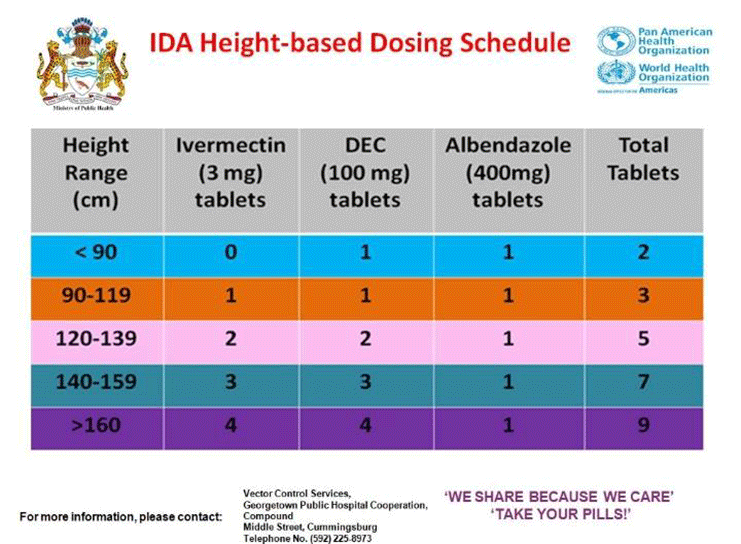
Before the MDA ends, however, three sets of pills must be taken. And there is a very specific dosing schedule that determines how many pills persons are required to take. All persons will be measured by trained pill distributors using a ‘dosing pole’ which measures from 90cm to 160cm. This dosing schedule is summarised in the table below:
This dosing schedule rigidly guides the distribution of the pills, and numerous studies done in other countries show the effectiveness of Ivermectin. “I understand persons may be worried about the pill burden, but even though they are worried about that, they shouldn’t be, because the pill burden is only high, based on the dosing schedule,” Dr. Sampson said, adding:
“Yes, we understand the pill burden, but we need to look at the bigger picture. Would I just want to look at the pill burden but not think about my health, if I am, in fact, infected with the worm that causes Lymphatic Filariasis?”
According to the WHO, Lymphatic Filariasis is a neglected infectious vector-borne disease that may be asymptomatic, acute or chronic. It may take several years, however, before the asymptomatic conditions develop into a chronic condition, which results in external manifestations of lymphoedema (tissue swelling), elephantiasis (skin/tissue thickening) of the limbs and hydrocele (scrotal swelling).
Importantly, Dr. Sampson stressed that these external manifestations are irreversible, and that there is no cure for the infection, which may take up to some 20 years before it manifests.
This is exactly what happened to Evelyn (not her real name) a few years ago. She was bitten by a dog, but noticed that two particular sores were not getting better, even when the rest had healed. After doing a plethora of medical tests, she was eventually advised to test for Lymphatic Filariasis.
“I went for three nights to do the test, and there it is when I got the results, it was Filaria,” Evelyn recounted recently. “I couldn’t believe it, because I was the one that was always careful; I used to use netting, I spray (mosquito repellant), mosquito coil, and what’s not,” she explained.
Since there is no cure for Lymphatic Filariasis, she enrolled in the Filaria Clinic at the Georgetown Public Hospital Corporation (GPHC), where she receives continuous treatment and even counselling.
THE CARE REGIME
On her own, she has adopted the ‘CARE’ regime which is used in tandem with the treatment she receives from the clinic. This regime involves: Cleaning the affected area, applying treatment, raising the affected area when sitting, and above the level of the head when lying down, and exercising.
In addition to being affected by filaria, Evelyn is also a vocal supporter of the MDA, because she believes that it was her failure to take the pills distributed previously that cost her. She disclosed that she was reluctant to take the filaria pills, despite encouraging her husband and children to take them.
“That was my neglect,” she said remorsefully, adding that some days the itching is unbearable while on other days, it is the pain that constrains her.
“Every time they (the pill distributors) come around, I will take what it is that they are giving us because I am telling you, it is not easy. I wouldn’t like nobody at all to get this thing because it is very painful,” Evelyn said.
This year’s MDA was launched at the end of October, and pills will be distributed to persons in Regions Three (Essequibo Islands-West Demerara), Four (Demerara-Mahaica), Five (Mahaica-Berbice) and Ten (Upper Demerara-Berbice) at various locations, including schools. Furthermore, as a result of the remapping exercise done in 2018-2019, the remaining six regions have been surveyed to ascertain their level of endemicity.
In Regions Eight (Potaro-Siparuni) and Nine Upper Takutu-Upper Essequibo), there is less than one per cent of endemicity, thus the MDA exercise is not required. For Region One (Barima-Waini), which was previously the only region that was endemic, the Moruca sub-region alone will be targeted, as will the entire Region Two (Pomeroon-Supenaam) except for Bethany and Dredge Creek. In Region Seven (Cuyuni-Mazaruni), only the town of Bartica will be targetted, while all of Region Six (East Berbice-Corentyne) will be targetted, except for Orealla and Sipuruta.
Dr. Sampson explained that once all of the regions have received and completed their treatment through the MDA, the country will then be able to start the process of being validated by the WHO, and subsequently direct focus to other public health issues.
“The impact and success of the IDA/MDA depends on the coverage; that is the total proportion of the population taking their pills. And that goes to say that the success of this campaign depends on you and me,” Dr. Sampson said.